
MAIN Blog
Rewilding Healthcare in Advanced Illness: An Invitation to Reimagine the Possibilities
In this post, Sarah Yardley, Associate Professor in Palliative Medicine and Honorary Consultant in Palliative Medicine, shares her reflections and experiences with MAIN
Rewilding Healthcare in Advanced Illness: An Invitation to Reimagine the Possibilities
People living with pre‑existing complex mental health conditions who also develop an advanced, incurable physical illness often experience distress that is not inevitable, but systemic.
Figure 1. Forms of intersectionality
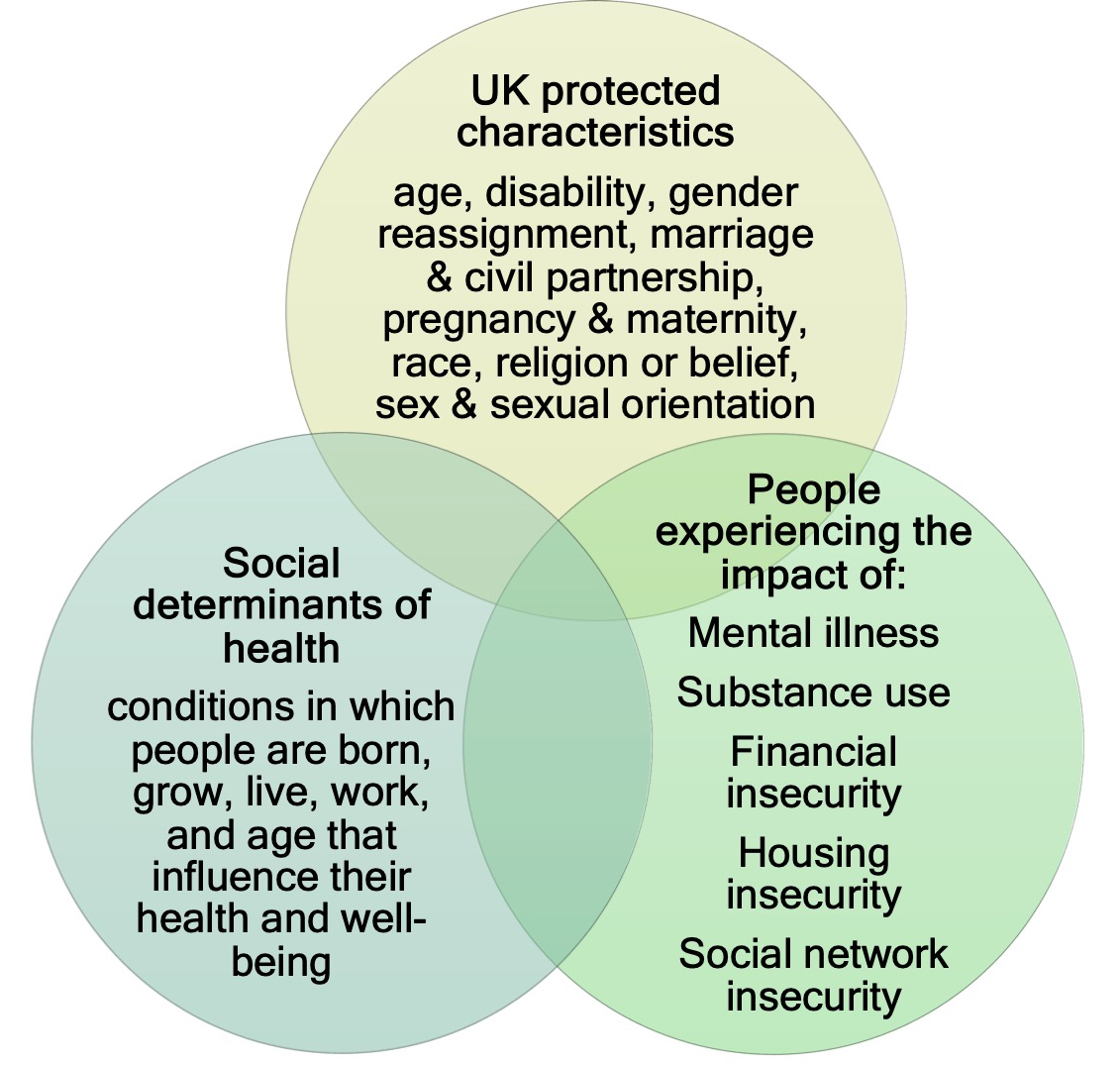
Figure 2. Part-system efficiencies
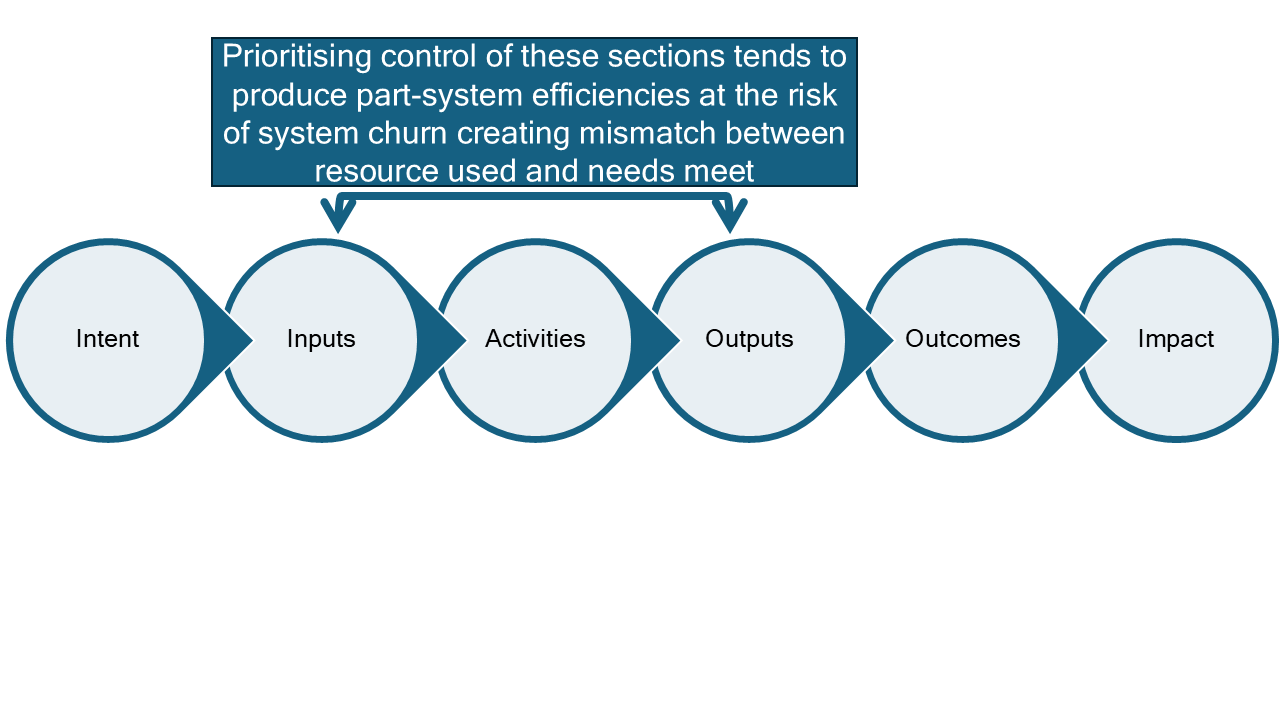
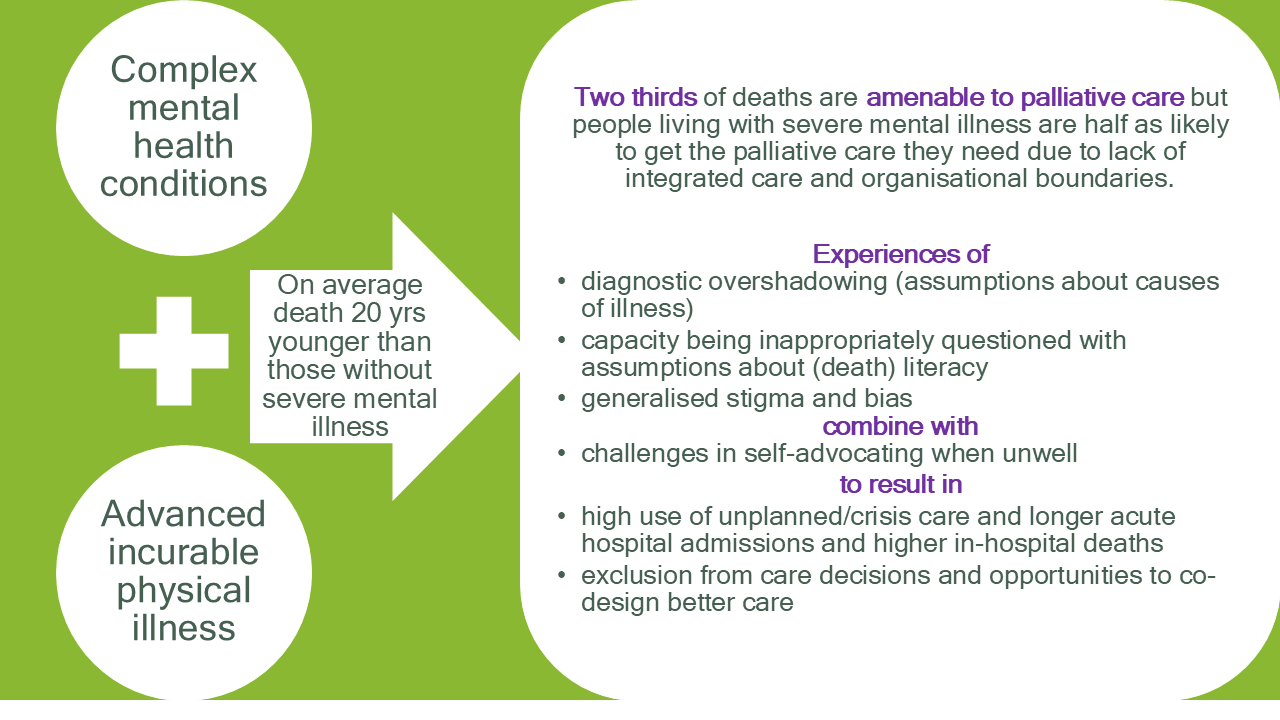
Figure 3. What is the problem?
I was awarded a Churchill Fellowship in 2024, funding my travel to learn from global innovators how palliative care can be reimagined for people with severe mental illness. Across the UK and internationally, I repeatedly heard versions of the same story:
“I don’t fit the system.”
“I’m treated differently.”
“When they see my mental health diagnosis, that’s it.”
These are not stories about individual failure; they are stories about structural vulnerability.
My Fellowship report, Rewilding Healthcare, explores what becomes possible when care ecosystems are redesigned so that relationships, not rigid structures, become the organising principle of palliative care for people with complex mental health conditions. Rather than asking when to use relational practice, the question becomes: How can we work relationally at every decision‑point?
Figure 4. Churchill Fellowship visits

Rewilding healthcare to cultivate systems that put relationship at the heart of care isn’t about creating a “wilderness”. It is about creating a balanced ecosystem of care with space for relational practices, focused on what matters most to people, and meeting their needs.
Why this matters for the MAIN community
This way of thinking aligns strongly with MAIN’s commitment to improving mental health and wellbeing in advanced illness, and with the network’s emphasis on research, evidence, psychological expertise, and cross‑sector collaboration.
MAIN’s Position Statement outlines clear priorities, from inequalities in access, to the importance of psychological support, to training needs, digital innovations, carers’ wellbeing, and stepped models of care. These priorities resonate deeply with the challenges described in my report: fragmented systems, delivery gaps, and the heavy reliance on “hidden work” that staff undertake to make care coherent.
What MAIN brings, and why this network is so valuable, is a research‑active, psychologically informed, interdisciplinary community. MAIN members include psychologists, clinical academics, palliative and mental health teams, social workers, lived‑experience partners, and policy colleagues. Together, this creates the conditions to move beyond describing the problem toward testing, evaluating, and sharing what works.
What the idea of Rewilding Healthcare offers
The report proposes that healthcare systems can be intentionally “rewilded”, not by removing structure, but by reshaping structures so they serve relationship and ecological resilience rather than controlling practice.
At its core, rewilding healthcare imagines care ecosystems where:
- Warm handovers replace referral chains
- Boundaries are permeable, allowing staff and trusted supporters to move with the person
- Psychological expertise and training are woven into everyday practice, not reserved for crises
- Distress is assessed universally, not only in those with a formal mental health diagnosis
- Coherence, not throughput, becomes a measure of success
Across the international sites I visited, systems that adopted these relational principles saw reduced crisis care and improved experiences — often without additional resources. Instead, effort shifted away from transactional processes and toward what genuinely meets people’s needs.
Figure 5. Recommendations for improvement
Three questions MAIN members may want to explore
I want to offer three reflective challenges that MAIN members, individually or collectively, may find useful as they read the report and consider how these ideas intersect with their practice, research, or teaching.
1. How “relationally ready” are the systems we work within?
Where are relational strengths already present, and where might small changes improve coherence, shared understanding, or responsiveness?
2. What might warm, relational handovers look like in our context?
How do we enable trusted relationships, peer supporters, carers, key workers, to travel with the person when care settings change?
3. How can psychological insight be shared more widely across teams?
Improving care for people living with complex mental health conditions depends on confidence, shared understanding, and psychologically informed practice across the whole workforce, not only among specialists. Academic partners within MAIN may be well placed to evaluate, adapt, and embed approaches that build this capability.
An invitation
I hope you will read the report through the lens of your own role, discipline, or research interests, and consider how its ideas might challenge, support, or inspire your work. If something resonates with you, unsettles you, or sparks an idea, I would love to hear from you.
Together, we can make relationship the mechanism of care, turning everyday contacts into steps that reduce distress, increase choice, and steward resources wisely.
Sarah Yardley, Churchill Fellow 2024

Email: Sarah.yardley@ucl.ac.uk
Related information:
- Dr Sarah Yardley’s academic profile
- Report: Rewilding healthcare by cultivating relational systems to reimagine palliative care
- The Churchill Fellowship is a UK charity which supports individual UK citizens to follow their passion for change, through learning from the world and bringing that knowledge back to the UK.
- Marie Curie Palliative Care Research Department
- UCL Division of Psychiatry

Published: Apr 07, 2026
Other blogs
- ‘I Love My Job’: Why We Need to Rethink Wellbeing Support for Healthcare Assistants in Palliative Care
- From Conversation to Collaboration: What happens after a MAIN Grant Planning and Networking Workshop?
- MAIN Grant Writing and Networking Workshop - Grant writing and creativity
- MAIN Grant Planning and Networking Workshop - Reflections and learning
- Welcome to our new blog site!
- Coming soon…